


Refractive surgery / Hyperopia
What is hyperopia?
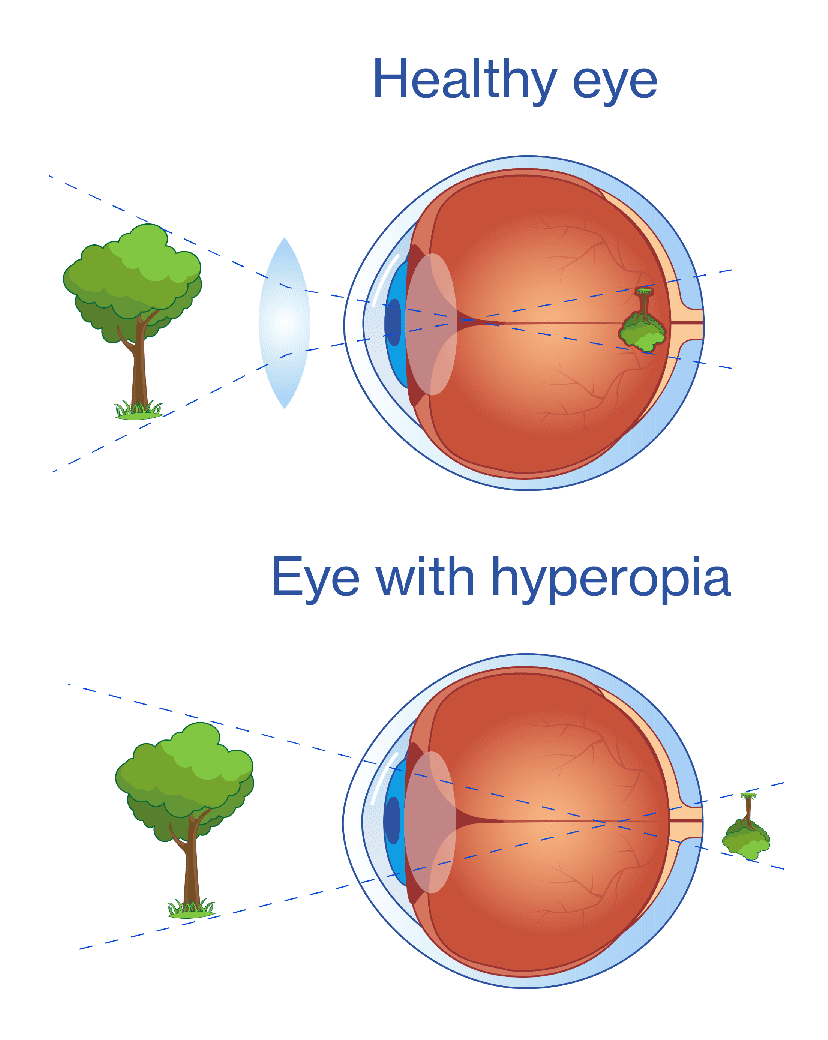
Hyperopia is an eye disorder that causes unclear and blurry vision when looking at objects close-up, as the images are focused behind the retina and not directly on it. As such, people suffering from hyperopia may have issues watching television, but they should be able to make out road signs, for example. If they have a very high prescription, objects in the distance may also appear blurry.
We all have hyperopia when we are born, but as our body develops, so do our eyes. If the eye does not grow as much as it should, the person will have hyperopia forever, unless it is corrected later after an examination by an ophthalmologist.
Hyperopia may occur on its own or in combination with astigmatism (hyperopic astigmatism).
Causes of hyperopia
Hyperopia occurs when the eye is shorter than it should be or because the cornea is too flat.
In patients with hyperopia, objects are focused behind the retina and not on it, as opposed to emmetropic patients (with 20/20 vision).
In young people, if the hyperopia is not too severe, it may be compensated by the eye muscles so the individual can see well at a distance and acceptably up close, but with age they will lose this ability and objects up close will lose focus, as will objects in the distance over time, which is known as presbyopia.
Although this disorder does not strictly increase with age, it may increase gradually (someone with hyperopia may have normal vision until 35-40 years old, and then it worsens as they get older), although the figure increases to 60% at 70 years old.
Symptoms of hyperopia
The effects of hyperopia are opposite to those of myopia. A patient with hyperopia will see worse close-up than at a distance. The higher the dioptres, the blurrier objects will appear close up. The most common symptoms suffered by patients with hyperopia are:
→Blurry vision
→Eye strain: this usually occurs in people with hyperopia after carrying out activities for prolonged periods of time that involve looking at something up close (e.g., working with a computer), spending time in poorly lit environments and/or physical or mental exhaustion, leading to visual discomfort.
→Headache: usually around the forehead area at the end of the day after excessive effort trying to focus the eyes. If the headache becomes more intense it can lead to nausea and vomiting.
→Convergent strabismus (when one eye turns inwards) may occur at times with people who suffer from hyperopia. When an object appears blurry to our brain, our nervous system involuntarily tries to accommodate the eyes in order to focus correctly. This attempt to accommodate the eyes can lead to a convergence reflex, where the eyes look inwards towards the nose, something entirely normal. When this convergence is excessive, it is classed as convergent strabismus. If we are able to make the issue go away through the use of glasses and the person has hyperopia, this is classed as accommodative strabismus.
→Red eyes at the end of the day.
Some cases of uncorrected hyperopia may also lead to blepharoconjunctivitis (which is a combination of conjunctivitis and blepharitis, or eyelid inflammation), but this is not common.
What is infantile hyperopia?
Infantile hyperopia usually occurs from the age of 4 years old, when the prescription is not too strong. However, it can be challenging to identify hyperopic vision, as the child will generally compensate their poor close-up vision by accommodating with their crystalline lens (the eye’s natural lens) to focus on objects.
That is why it is particularly important for children to undergo regular examinations from an early age, so they can work with the ophthalmologist to detect any infantile refractive disorder early.

Symptoms: How to identify infantile hyperopia
With newborns it is a very common disorder that tends to resolve by itself over the first few months of life, as our visual system is not fully developed when we’re born
However, if it does not resolve itself, hyperopia in children should be identified as early as possible as it not it can lead to what is known as lazy eye (poor vision in one of both eyes due to lack of use during development of the visual system, as the child prioritises the eye with less refractive issues) or infantile strabismus, particularly if the strabismus is convergent (the eye turns inwards). This can be fully or partially corrected.
The importance of early diagnosis in hypermetropia
Teachers and parents play a fundamental role in identifying this refractive issue as it can present itself in the following ways:
→The child has problems reading or writing.
→Poor performance at school, bad grades of problems concentrating.
→Eye strain.
→Red, watery or itchy eyes, which may cause the child to rub their eyes, blink excessively or frown.
Treatment for hyperopia in children
If infantile hyperopia does not disappear during adolescence, the ophthalmologist will consider correcting their vision through the use of glasses, particularly if the hyperopia is severe and is causing other symptoms. Furthermore, depending on the age of the child, the ophthalmologist may consider correcting the child’s hyperopia with contact lenses if they have issues performing certain activities, such as playing sports, or in cases of anisometropia, where there is a significant difference in the prescription of each eye.

Hyperopia: classification
Hyperopia
curve
This applies to cases where the radius of the first side of the lens is smaller than that in the emmetropic eye.
Hyperopia
axial
This is when the optical axis is shortened.
Index of
hyperopia
This is due to an increase in the refraction index of some of the transparent elements in the eyeball.
Latent
hyperopia
This is when the ciliary muscle is used to compensate for the hyperopia.
Pronounced
hyperopia
This is where the ciliary muscle does not compensate for the hyperopia, and it is classified into the following three types:
→Facultative hyperopia: the patient can compensate for the hyperopia with accommodative effort.
→Absolute hyperopia: the patient does not compensate for the hyperopia with the ciliary muscle or with accommodative effort.
→Total hyperopia: this is a combination of facultative and absolute hyperopia, so it is the most severe type.
Types of hyperopia
THE MOST COMMON
Simple
hyperopia
This is the most common kind. It is generally a continuation of infantile hyperopia that has become chronic, meaning that one eye has not developed properly (the anterior-posterior axis of the eyeball has reduced).
Combined
hyperopia
This is when the vitreous becomes shorter and the cornea becomes flattened.
Mixed
hyperopia
This is when the cornea is flat and the vitreous is longer, or the cornea is more curved and the vitreous is shorter.
Hyperopia surgery
Myopia can be corrected with glasses and/or contact lenses, and also through refractive surgery. Although it is true that for those with medium-high hyperopia, adapting to their prescription may be difficult, as there will be a reduction in their visual field (usually starting from around 6 dioptres).
To correct the patient’s vision permanently, once their prescription has been stabilised, we can perform eye surgery. But before performing hyperopia surgery, the ophthalmologist will perform a full ophthalmology examination to assess the condition of the eye and the thickness of the corner, in order to determine the most suitable technique for the patient.
How is hyperopia diagnosed?
At Oftalvist we believe that the first consultation should not be merely informative, it should be a visit where the patient goes home knowing if their hyperopia can be corrected and which technique would be most suitable, after we perform the following pre-operative tests:
✓Measurement of intraocular pressure.
✓Test for visual acuity and prescription.
✓Examination and diagnosis of the anterior and posterior segments of the eye.
✓A detailed examination of the eyes: laser biometry, corneal topography, aberrometry and corneal pachymetry.
Once we have obtained the results, the most common surgical treatments are as follows:
→Laser refractive surgery (or Lasik) performed with a femtosecond laser: this technique is used most often due to its proven safety and effectiveness. It involves modifying the shape of the cornea with a laser to change the total refraction of the eye.
→Intraocular lens implant (phakic): this is offered for select cases (without removing the crystalline lens). This is a painless and very safe outpatient surgical procedure performed using local anaesthetic. It corrects hyperopia at a range of +0.5D to +10.0D, with or without astigmatism of up to 6.0D.

